Study Based on Nearly 10,000 Infected People in Shanghai: Domestic Vaccine Significantly Reduces Rates of Serious Illness in the Elderly
Read Time:6 Minute, 18 Second
How effective is the domestically produced inactivated new crown vaccine?
On December 8, the surging news reporter learned from the Jiaotong University School of Medicine that recently, Chen Saijuan’s team from Ruijin Hospital and the National Major Infrastructure for Translational Medicine (Shanghai), affiliated with Jiaotong University School of Medicine, and Professor Fan Xiaohong’s team from Shanghai Public Health Clinical Center (hereinafter referred to as the Public Health Center) launched a joint research study and published a paper in Frontiers of Medicine titled “Host protection against Omicron BA.2.2 sublineage in spring 2022 outbreak in Shanghai”. The research paper entitled “Host protection against Omicron BA.2.2 sublineages by prior vaccination in spring 2022 COVID-19 outbreak in Shanghai” was published in Frontiers of Medicine, which summarized and analyzed the clinical characteristics of 9,911 infected patients admitted to the Public Health Center during the outbreak, as well as the inactivated vaccines produced in China, revealing the clinical molecular characteristics of BA.2.2 infection and the inactivated vaccines received. The clinical characteristics of the 9,911 infected patients admitted during the outbreak and the vaccination with our own inactivated vaccine were summarized and analyzed to reveal the clinical molecular characteristics caused by BA.2.2 infection and the protective effect of the vaccinated New Crown vaccine.
Published papers
The Omicron mutant strain has caused several rounds of large-scale outbreaks around the world since its emergence in November 2021 due to its superb transmission and immune escape ability. During its transmission, the Omicron genome sequence also continues to accumulate mutations, gradually generating major sublineages such as BA.1, BA.2, BA.3, BA.4, and BA.5, as well as multiple subbranches under each sublineage. The high diversity and infectiousness of these new coronavirus variants pose a great challenge to public health health and epidemic prevention measures.
The two aforementioned teams noted that in the first half of 2022, the Omicron BA.2.2 sublineage strain (referred to as BA.2.2) that caused the wave of the epidemic was imported into Shanghai from outside the country and rapidly caused large-scale community transmission, resulting in a cumulative total of 649,354 infections, of which 591,349 cases (91.06%) were asymptomatic, and 588 cumulative deaths (0.09% mortality).
Based on epidemiological analysis, a low proportion of severe and critically ill cases (2.76%) were found among symptomatic neocoronavirus infected patients, mainly in the elderly population aged 60 years or older. The rate of severe disease was about 0.2% among socially oriented neo-coronavirus infected patients, including asymptomatic infected patients.
Grouping patients by age revealed that the rate of severe and critical illnesses increased progressively with the age of patients, but the rate of severe illnesses in the vaccinated population in each age group was significantly lower than that in the unvaccinated population, and the degree of reduction was highly correlated with the number of vaccination doses.
For example, in the three age groups of 60-69, 70-79, and ≥80 years, the rates of severe and critical illness in unvaccinated patients were 8.64%, 17.12%, and 20.28%, respectively; the rates of severe and critical illness in 1-dose vaccinated patients were 6.90%, 12.12%, and 14.29%, respectively, and the rates of severe and critical illness in 2-dose vaccinated patients were 0.76%, 4.76% and 4.35% for patients with 2 doses of vaccine, and 0.58%, 2.60% and 0.00% for patients with 3 doses of vaccine, respectively.
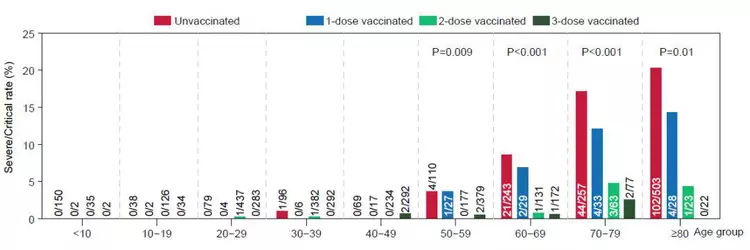
Number and proportion of severe cases among newly crowned patients with different doses of vaccine by age group
The team therefore concluded that even though older people were more likely to develop severe and critically ill neocon disease, 2-3 doses of inactivated vaccine in symptomatic infected individuals still provided 90.15% protection against severe disease in patients over 60 years of age (96.02% protection against severe disease in all patients).
Second, analysis of peripheral blood samples from BA.2.2-infected patients revealed that abnormal changes associated with disease progression (e.g., anemia, abnormal coagulation indicators, organ damage, etc.) were protected to varying degrees in vaccinated patients, especially lymphocytopenia associated with severe and critical illnesses, which was well relieved in vaccinated patients: routine blood tests showed that in severe/ In critically ill cases, peripheral blood lymphocyte counts returned to near-normal levels 16 days after admission in patients who had received Neocrown vaccine, whereas lymphocyte counts in non-vaccinated patients remained below normal levels for 30 days.
In addition, by comparing the clinical data of 963 patients with new coronavirus admitted to public health centers during the BA.2.2 and 2020 epidemics of the prototype strain of new coronavirus, it was found that the median age of patients with severe and critical illness in those infected with BA.2.2 in the 2022 spring epidemic in Shanghai was 81 years (range: 72-89 years), whereas the median age of patients with severe and critical illness in those infected with the prototype strain during 2020 age was 64 years (range: 55-71 years). Using the normal range of all clinical tests as a reference, the overall baseline health status of BA.2.2-infected patients with severe and critical illnesses was already lower than that of patients with severe and critical illnesses infected with the prototype strain at the beginning of their admission.
Taken together, the results of these analyses show that 2-3 doses of inactivated neo-coronavirus vaccine can effectively prevent progression from mild or common clinical manifestations to severe disease in neo-coronavirus-infected patients, and also have a significant effect on reducing the rate of severe disease in the elderly population over 60 years of age, and these results are consistent with recent analyses of mRNA vaccine efficacy in several countries and regions.
It is worth mentioning that the previously approved New Crown vaccine for some populations with underlying diseases, such as advanced age, three highs (hypertension, hyperlipidemia, hyperglycemia), diabetes, autoimmune deficiency diseases, uremia, and tumors, is recommended to be withheld. Since these underlying diseases are mainly concentrated in the elderly population, the overall vaccination rate for this group has been low so far.
As of November 14, 2022, only 46.19% of the population aged 60 years or older in Shanghai had still completed three doses of vaccination, according to Saijuan Chen. However, this study shows that the elderly population is precisely the most high-risk group for neo-crown severe disease that should receive vaccination, “redefining scientifically the contraindications to vaccination, promoting comprehensive neo-crown vaccination and vaccination as needed, especially further promoting vaccination of high-risk groups for neo-crown with stable control of underlying disease, will be an Effective method.”
Fan Xiaohong also pointed out that, at present, it is important to promote the approval of new iterations of vaccines and vaccination programs, and do a good job in the production stockpile and clinical use of anti-neo-coronavirus drugs (especially small-molecule targeted drugs) and adjuvant drugs, as well as Chinese medicine with definite efficacy; implement classification and stratified treatment, with medical observation and treatment centers moved down for asymptomatic and generally mild patients and designated hospitals for serious patients, while strengthening individual family knowledge and skills of prevention and control The final victory in the fight against the epidemic will be achieved through the popularization of individual family prevention and control knowledge and skills, good health promotion and risk communication, and the compacting of responsibilities of all parties.
Happy
0 %
Sad
0 %
Excited
0 %
Sleepy
0 %
Angry
0 %
Surprise
0 %


Average Rating